WEISS 2014 投射认同的五阶段模型 - 5

王静华2016-4-19 15:13
查看:2730次
“趟过”蒙利·凯里反移情之转化修通、比昂的容器/涵容物、梅兰妮·克莱因未公开发表的投射性认同,接下来终于到了Heinz Weiss 海因兹·韦斯提出的五阶段模型了
A multiphase model of projective identification
投射性认同的多阶段模型
Taking
up Melanie Klein’s thoughts as outlined above, the first step is an attribution, i.e. a binding of the projection to the
analyst, before the second step of getting into his internal world takes place.
According to Klein, it makes sense to distinguish these two part processes in
clinical technique. The first attributional phase could be described as adhesion.
使用梅兰妮·克莱因的观点,第一步是归因,也就是在第二步、进入病人内部世界之前,病人先将投射粘附于分析师。克莱因认为,在临床技术上区分开这两个步骤是有意义的。第一步归因阶段可以被描述为粘附。
First phase: Adhesion
第一个阶段:粘附
The
projective identification (P) must reach the analyst (A), i.e. it must adhere to his psychic surface. This happens
by way of feature or characteristic trait of the analyst, which matches the
particular projection. The corresponding feature could be called the point of
adhesion or the receptor
(R), where the projection
adheres (see Figure 1). A connection between the psyche of the analyst and the
projection of the patient is forged, which is more than just a reflection on an
opaque “mirror” (Freud, 1912, p. 118).
投射认同(P)必须达到分析师(A),也就是必须粘附在分析师的精神表层。这一步的发生是分析师的外貌或性格特征可以匹配特定的投射。对应的特征被称为粘附点或者是投射粘附的受体(R)。(见图1)。
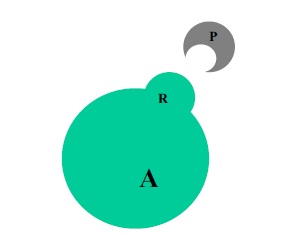
Fig. 1. Adhesion of the projection 图1 投射粘附
However,
in this phase the internal world of the analyst is not fundamentally affected.
He experiences the projective identification as originating from outside, i.e. as a two-dimensional adhesive projection.
This corresponds with projective identification
as projection (see Sandler, 1987) or as omnipotent phantasy (Feldman, 1997; Klein, 1946). These do not necessarily disturb the analyst
even though they may contain very disturbed and even psychotic elements.
Rosenfeld (1971) and Bion (1958) have described such projections, which do not
lead to a marked “involvement” of the analyst (see Feldman, 1997, pp. 229–30), and can therefore be interpreted in a
relatively direct way. B. Joseph (1987) has also pointed out that the way and
degree of being influenced by projective identification may vary considerably.
In this sense, Feldman (1997, p. 230) distinguished between projective
identification, which leads to an enactment, and projective identification as a phantasy, which does not permanently
alter the internal state of the analyst.
可是,在这个过程中,分析师的内部世界并没有被根本性地影响。他体验到投射认同是来自于外部世界,也就是作为二维的投射粘附。这对应于投射性认同是投射(桑德勒, 1987)还是全能幻想(费尔德曼, 1997; 克莱因, 1946)。这些不一定会使分析师混乱,即使可能包含非常扭曲的乃至精神病性的元素
。罗森菲尔德(1971)和比昂(1958)已经描述过这类投射并没有导致分析师显著的“卷入”(罗森菲尔德, 1997, pp. 229–30),因而能够以相对直接的方式进行诠释。B.约瑟夫(1987)也指出被投射认同影响的方式和程度可能变动非常大。针对这一点,费尔德曼(1997,p.230)区分了导致付诸行动的投射性认同与作为幻想的投射性认同,后者没有持久地改变分析师的内部状态。
There
are different views as to whether it is meaningful to distinguish between
intrusive and non-intrusive projective identification or indeed whether there
is anything like a non-intrusive projection. Clinically,
there seem to be different grades of intrusiveness which influence the reaction
of the analyst and his capacity to interpret in different ways. Maybe Melanie Klein’s
advice to advance the interpretations ‘step by step’ in tune with the feelings
and anxieties evoked in the patient can be understood in this sense.
侵入性投射认同、非侵入性投射认同或者甚至任何类似于非侵入性投射,对它们进行区分是否是有意义的、持有不同的观点。临床上,看起来有不同的侵入程度,这会影响分析师的反应和他以不同方式进行解释的能力。从这个意义上来讲,克莱因建议根据病人诱发的感觉和焦虑程度“一步一步”地进行解释就可以理解了。
Problems in the area of the first phase
第一阶段存在的问题
Problems
could arise either because there is no place to adhere to or too strong and too rigid an adherence is formed between the projection of the patient
and the place of adherence in the analyst. In the former case, the patient will
have the feeling that he cannot reach the analyst. The analyst in turn will
find it difficult to make an emotional link with the material of the patient so
that he can only have a limited experience of the meaning of the material
within the transference situation. In the latter, the link will be too tight,
i.e. the projection will stick to the psychic surface of the analyst and appear
as its natural equivalence. In this case it will be difficult to interpret the
projection as something emanating from the patient: the patient feels confirmed
in his projective phantasies by certain characteristics of the analyst. The
analyst in turn finds it difficult to recognize the patient’s projections behind
the initially apparently ‘realistic perceptions’.
If this is very marked, the projection has probably gone very deep into the
analyst and will be identified with one of his internal objects.
无处粘附或者是病人投射与分析师粘附位置之间太强太硬都意味着出现了问题。前者,病人会感觉无法触及分析师;而分析师也会觉得很难与病人的材料之间建立有情感的连接,以至于他只能在移情位置上很有限地体验到材料的意义。后者,连接太强了,也就是投射粘在分析师的精神表层、就好像它很自然而然在那儿的。在这种情况下,很难对源自病人的投射形成解释:病人在其投射性幻想中被分析师的某些特征感到被加强了;而分析师发现难以从他起初明显地“现实感知”背后识别出病人的投射。如果这非常明显,说明已经很深地投射进分析师内并且将和分析师的内在客体之一形成认同。
Interpretation
解释
At best – when the projection adheres, but not too rigidly
– the analyst will be able to interpret the
projective phantasy as something that is taking place ‘outside’ him, so to say.
It is doubtful though whether this kind of relationship ever exists in this
pure form or whether there will be some form of intrusion even at this stage.
However, the penetration will not be very forceful, i.e. less dependent on
repudiation and splitting of parts of the self and more likely of a transient
nature, such as described by Joseph (1987), for example, in patients who are
getting close to the depressive position. Ideally, the analyst will maintain
his more or less observational stance, i.e. the patient will not stay ‘inside’
him. Through the interpretation the emerging
connection will be analysed. The patient will be able to
take back his projection and recognize it as something emanating from him. For
example, this will be the case in classic transference interpretations. However, most of the time,
the projection intrudes into the analyst and affects his countertransference. This receptive function of analytic
understanding was probably what Freud meant when he required that the therapist
“must turn his own unconscious like a receptive organ towards the transmitting
unconscious of the patient” (1912, p. 115).
最好的情况是——投射粘附在那儿,但不是太坚固——可以这么说,如同是在他“之外”发生的,分析师可以有能力解释投射性幻想。不能确定的是,这种关系是否存在这么纯粹的形式还是说即使在这样的一个阶段也有某种形式的侵入。可是,穿透不会是非常强有力,也就是说不取决于部分自体的否认和分裂,而更像是约瑟夫(1987)描述的是一个、如病人正接近抑郁位的短期状态。理想情况下,分析师将或多或少地维持着观察者的立场,也就是说病人不会驻留在分析师“里面”。浮现出来的联结通过解释而被分析。病人就能够收回投射并承认这是源于他自己的部分。可是,大多数情况是,投射侵入分析师内并影响分析师的反移情。分析性理解的接纳性功能可能就是弗洛伊德要求的,他要求分析师“必须将他自己的无意识作为病人的无意识传递的接受器官。”